
Dr. Benjamin Boublil
View ProductCase 1:
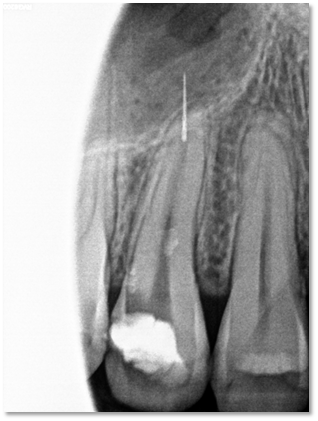
The tip of the broken instrument was only one mm in. I found the file wasn't really engaged in the dentine, and activating a loose instrument on its external aspect can easily have it projected out in the apical direction. Since we tried not to go for a surgery for this particular patient, for comfort reasons, proper care and CBCT analysis are crucial. Placing your sharpened TFRK tip on the side facing the curvature and activating in the presence of EDTA, and the instrument will come out immediately.
Case 2:


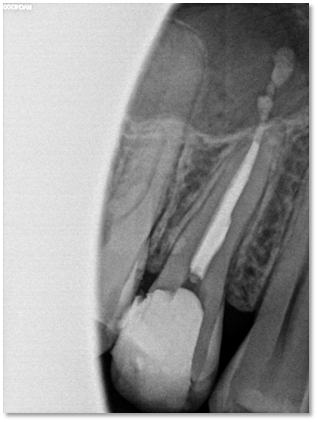
S shaped canal vs long separated file. The file is usually only engaged with its coronal portion, being more tapered. Martensitic instruments will come out easily, since they have less resting form. A previous attempt of removal had been done by the referring dentist, so access to the coronal tip was made easier. Identify the inward curvature side, often mesial and lingual for a MB canal, through till it moves, then grab it out! Activating the lubricating solution sure helps.
Case 3:



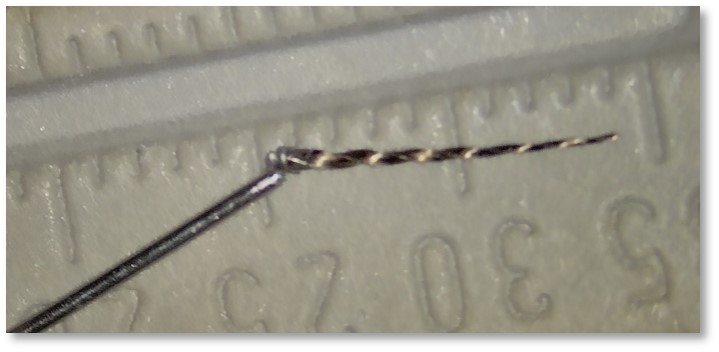
Easier case, as the instrument is shorter and the canal rather straight. Most of the job is done with CBCT analysis, I sometimes like to sketch the situation so I don't have to go back to the CT while I'm working. I'd write : 4 mm buccal instrument, 7 mm deep, go inside-inside, and keep the doodle on a post-it note close by. Activate the tip on the right side with EDTA, and loop it out quickly.
Case 4:


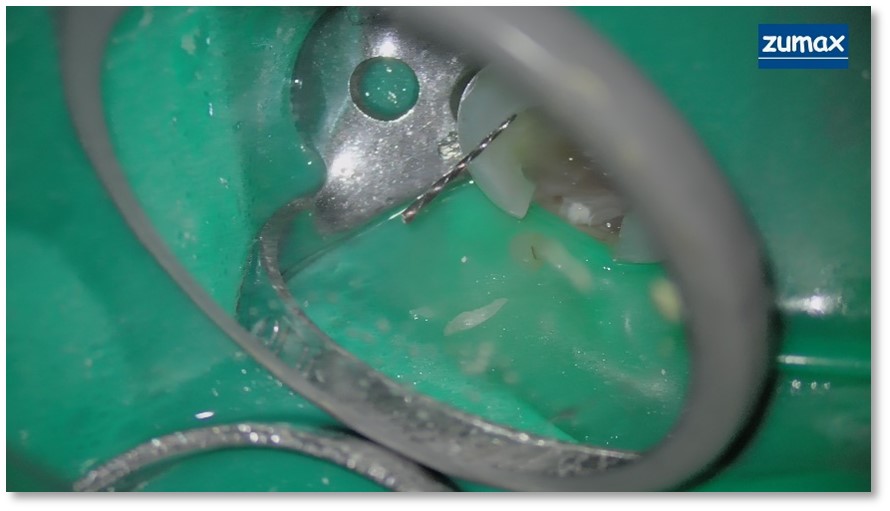
For this deeper placed fractured instruments, I used a F5 until contact was felt on the coronal part of the BI. Austenite files will require more throughing, time and patience. If it not visible, tactile sense must be used to avoid perforation and excessive sound dentine removal. I used a semicircular prep in the presence of EDTA, in the wall facing the curvature. Once the tip of the TFRK feels 'sticky', activate with up and down motions, until the instrument comes out. Being not visible, I did not use a loop here, the prep was enough
Case 5:


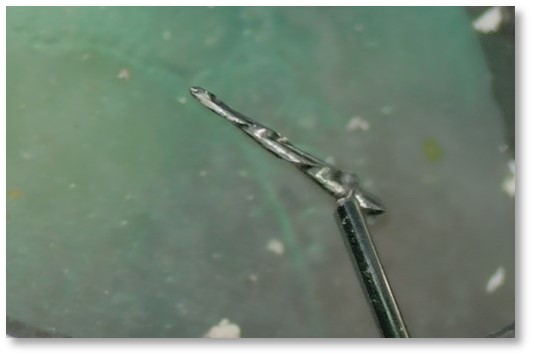
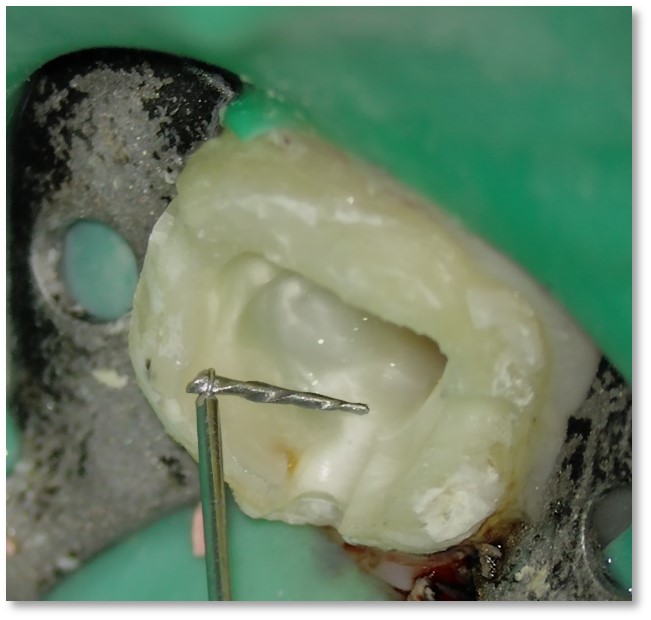
After enlargement of the canal with a #2 modified GG drill and access to the tip of the fractured file, a semi-circular prep is achieved with a TFRK tip. This takes time, to avoid over throughing, and after a while, in presence of EDTA, the broken instrument began to move up and down. It was an easy grab with the TFRK Loop+.